Presentation by Dr. Alan Kaye (Advanced Radiology Consultants) at ACR 2013 Imaging Informatics Summit, quoting Dr. Rawsson: “It’s hard to put the patient at the center of the universe if you’re sitting there yourself.”

Presentation by Dr. Alan Kaye (Advanced Radiology Consultants) at ACR 2013 Imaging Informatics Summit, quoting Dr. Rawsson: “It’s hard to put the patient at the center of the universe if you’re sitting there yourself.”
The benefits will come, but we must get through the change and this will be painful. Think of the shift from film to filmless, and paper to paperless (with coded, structured records) is this, times a thousand.
When I think about how much effort is put into ensuring the right info gets associated with the right patient in standards and interoperable records, the thought that a patient’s clinical info could be “corrupted” through copy-paste by users is very scary.
Like many problems, there are more than one valid solution. For the challenge of getting images to both diagnostic consumers (e.g. Radiologists) and clinical consumers (e.g. ordering physicians, EMR users), there are many ways to define a solution architecture, but two are most obvious: PACS-centric and VNA-centric.
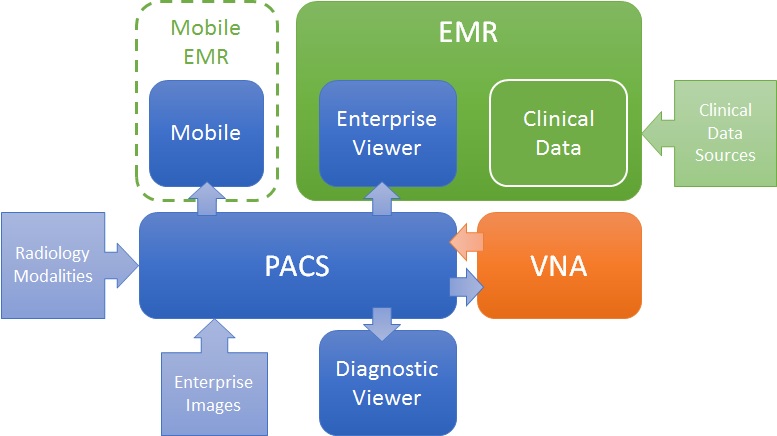
PACS-centric
In this model, the PACS is the primary system, interfacing with modalities, providing a client to diagnostic users, as well as access to clinical users though an enterprise client embedded in the EMR. Mobile access may be direct or via a mobile EMR user interface, but it is getting images from the PACS. Enterprise images are captured and stored in the PACS (though storing to VNA and routing to PACS is also possible). The VNA’s role is primarily as an archive to (one or more) PACS.
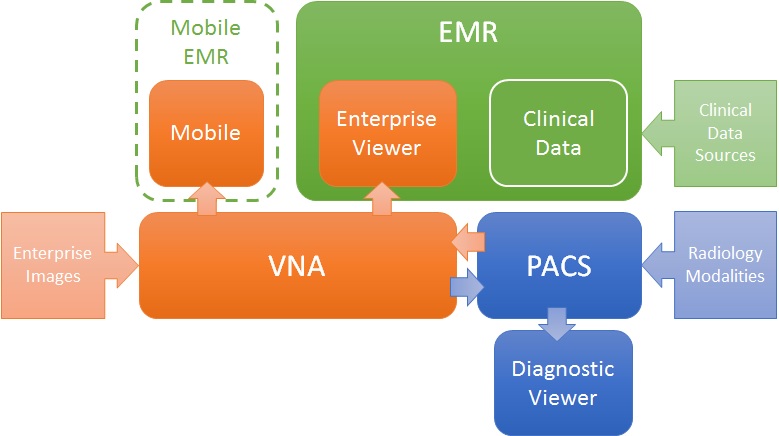
VNA-centric
In this approach, the VNA is the primary image management system. The PACS likely still interfaces with modalities (though not always), but captured enterprise images are stored to the VNA, and sent to the PACS when needed/supported. Clinical viewing in the EMR is done by an Enterprise Viewer, which may or may not be provided by the VNA vendor. Mobile access is also through the Enterprise viewer, getting images from the VNA.
Pros and Cons
As stated, both are valid approaches, but each has some inherent strengths and challenges.
The PACS-centric solution has a high likelihood of having all parts of the medical imaging record being available in both diagnostic and enterprise viewers. Proprietary data (e.g. markups and key images) not provided through standard data objects (e.g. DICOM GSPS and KOS) are more likely to be visible in all clients. There may also be some common application configuration settings across clients, which would reduce administration complexity and cost. Getting the image management and image viewing (diagnostic and enterprise client) all working together is the burden of the vendor (i.e. it is an engineered solution designed to function as a single system).
The VNA-centric solution is better suited to support a multi-PACS environment, providing a common management and viewing platform for enterprise users—only the single Enterprise Viewer is embedded in the EMR (vs. the multiple ones provided by each PACS). Environments with multiple PACS and Mini-PACS benefit as the VNA is the common sharing (and data quality validation) point among them—this allows for a more “pluggable” solution where systems that address niche needs can be used until the primary PACS is able to replace them. In this model, the integration among the components is more complex and places a higher burden on the institution to get it all working (i.e. the informatics and IT staff need to be willing and able to put this together), even with purchased professional services from all the vendors involved.
Assuming both the PACS and the Enterprise Viewer support LDAP (Lightweight Directory Access Protocol) and/or SSO (Single Sign-On), user authentication may be equal in both approaches.
Both a well-designed PACS and VNA (and Enterprise Viewer) can provide effective multiple patient ID management methods (e.g. MPI or IHE Patient Identifier Cross-Referencing), to allow integration/exchange of patient imaging records across patient ID domains, though the VNA and Enterprise Viewer are traditionally more likely than PACS to support flexible models.
In both models, storage for the long term archive is expanded at the VNA.
I find the topic of this article interesting.
Here’s why…
Check out this article. Some fairly common observations for an IT veteran, but good advice for EHR buyers.
Some mitigation tips for each point (read the article for the 4 hurdles)…
In regards to the comments on the trade off of lost productivity vs. potential new revenue, check out this post from a month ago.
The news from today (May 2013) “Quebec to expand $1.6 billion EHR“. And, from 24 months ago (May 2011), “Quebec’s EHR late and over budget, AG says“.
One thing is for sure: implementing an EHR of that size and scale (with public funds), is not for the faint of heart.
A friend forwarded this article on to me. It is great to see the energy being put into innovation in healthcare IT—it certainly needs it.
I have attended a few talks on the challenges facing start-ups when entering the realm of healthcare applications. Not only is healthcare a complex domain, with established vendors too often hoarding data in closed systems, but the whole issue of potentially having to becoming a registered medical device manufacturer can be daunting. I am hoping that some entrepreneurs with experience in regulatory affairs and quality system management emerge to provide affordable consulting services to start-ups. Full-time regulatory staff are often expensive and bureaucratic.
I have a written a couple of papers on innovation in different sized companies and environments. They will be published in the next few months. Stay tuned.
Earlier this week I posted an article on Accountable Care. Well, here is part 2. Check it out.
The “business” C’s (from the article)…
As I mentioned last week, there was some valuable info shared at the Apps for Health event at Mohawk college in Hamilton.
The keynote speaker, William Falk (@willfalk), shared some valuable statistics, along with a proposal for how to envision different types of apps, using a pharmacy dispensing different types of drugs, as a metaphor.
He has also shared his slides, which are well worth a look. Enjoy.
