In my previous post, I discussed common challenges associated with the imaging exam acquisition workflows performed by Technologists (Tech Workflow) that many healthcare provider organizations face today.
In this post, we will explore imaging record Quality Control (QC) workflow.
Background
A typical Consolidated Enterprise is a healthcare provider organization consisting of multiple hospitals/facilities that often share a single instance of EMR/RIS and Image Manager/Archive (IM/A) systems, such as PACS or VNA. The consolidation journey is complex and requires careful planning that relies on a comprehensive approach towards a solution and interoperability architectures.
An Imaging Informatics team supporting a Consolidated Enterprise typically consists of PACS Admin and Imaging Analyst roles supporting one or more member-facilities.
Imaging Record Quality Control (QC) Workflows
To ensure the quality (completeness, consistency, correctness) of imaging records, providers rely on automatic workflows (such as validation by the IM/A system of the received DICOM study information against the corresponding HL7 patient and order information) and manual workflows performed either by Technologists during the Tech Workflow or by Imaging Informatics team members post-exam acquisition. Automatic updates of Patient and Procedure information are achieved through HL7 integration between EMR/RIS and the IM/A.
Typical manual QC activities include the following:
- Individual Image Corrections (for example, correction of a wrong laterality marker)
- DICOM Header Updates (for example, an update of the Study Description DICOM attribute)
- Patient Update (moving a complete DICOM study from one patient record to another)
- Study Merge (moving some, or all, of the DICOM objects from the “merged from” study to the “merged to” study)
- Study Split (moving some of the DICOM objects/series from the “split from” study to the “split to” study)
- Study Object Deletion (deletion of one or more objects/series from a study)
QC Workflow Challenges
Access Control Policy
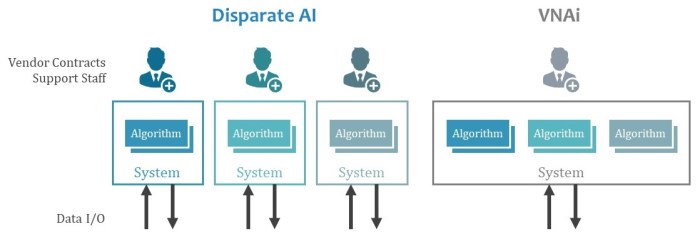
One of the key challenges related to ensuring the quality of imaging records across large health system enterprises is determining who is qualified and authorized to perform QC activities. A common approach is to provide data control and correction tools to staff from the site where the imaging exam was acquired, since they are either aware of the context of an error or can easily get it from the interaction with the local clinical staff, systems, or the patient themselves. With such an approach, local staff can access only data acquired at sites to which they are assigned to comply with patient privacy policies and prevent any accidental updates to another site’s records. The following diagram illustrates this approach.

Systems Responsibilities
Another important area of consideration is to determine which enterprise system should be the “source of truth” for Imaging QC workflows when there are multiple Image Manager/Archives. Consider the following common Imaging IT architecture, where multiple facilities share both PACS and VNA applications. In this scenario, the PACS maintains a local DICOM image cache while the VNA provides the long-term image archive. Both systems provide QC tools that allow authorized users to update the structure or content of imaging records.

Since DICOM studies stored in the PACS cache also exist in the VNA, any changes resulting from QC activity performed in one of these systems must be communicated to the other to ensure that both systems are in sync. This gets more complicated when many systems storing DICOM data are involved.
Integrating the Healthcare Enterprise (IHE) developed the “Imaging Object Change Management (IOCM)” integration profile, which provides technical details regarding how to best propagate imaging record changes among multiple systems.
To minimize the complexity associated with the synchronization of imaging record changes, it is usually a good idea to appoint one system to be the “source of truth”. Although bidirectional (from PACS to VNA or from VNA to PACS) updates are technically possible, the complexity of managing and troubleshooting such integration while ensuring good data quality practices can be significant.
The Takeaway
Often the QC Workflow is not discussed in depth during the procurement phase of a new PACS or VNA. The result: The ability of the Vendor of Choice’s (VOC) solution to provide robust, reliable, and user-friendly QC tools, while ensuring compliance with access control rules across multiple sites, is not fully assessed. Practice shows that vendors vary significantly in these functional areas and their capabilities should be closely evaluated as part of any procurement process.