In my previous post, Dealing with Multiple Terminology Domains in a Consolidated Enterprise, I introduced a typical challenge that many imaging projects face today.
In this post, I will describe three common use cases where the problem of multiple terminology domains manifests.
Single PACS, Multiple RIS
Often, rapidly growing health systems aim to consolidate imaging informatics solutions across their facilities. Replacement of multiple PACS with one such system, while keeping separate RIS systems in place is not uncommon. The reason behind this dichotomy is that a RIS is much more ingrained into the local Radiology department’s operational and clinical workflows than a PACS, making its replacement complex and impactful on many stakeholders.
The following diagram illustrates this scenario.
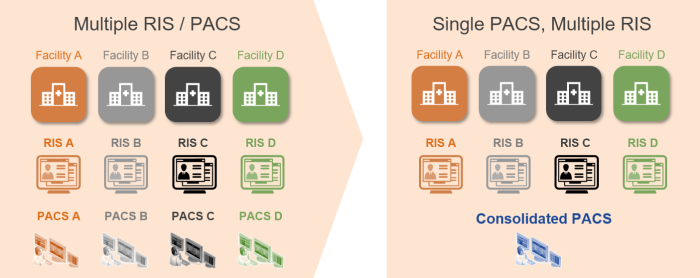
In such a deployment, the consolidated PACS is responsible for dealing with multiple ordering systems that use individual procedure terminologies. It also maintains patients’ longitudinal imaging record, which will include different values in the DICOM headers to describe the same procedure types.
Multiple RIS/PACS, Shared VNA
Health systems that seek to benefit from IT infrastructure consolidation, as well as a single Imaging Record Management, Archive, Access, and Sharing application, often opt to procure and deploy a shared VNA system across their facilities. By keeping their RIS/PACS systems in place they can rapidly deliver clinical and operational benefits with minimal disruption to the existing workflows. This approach allows individual facilities to stay fairly independent in their imaging informatics system and process decision making.
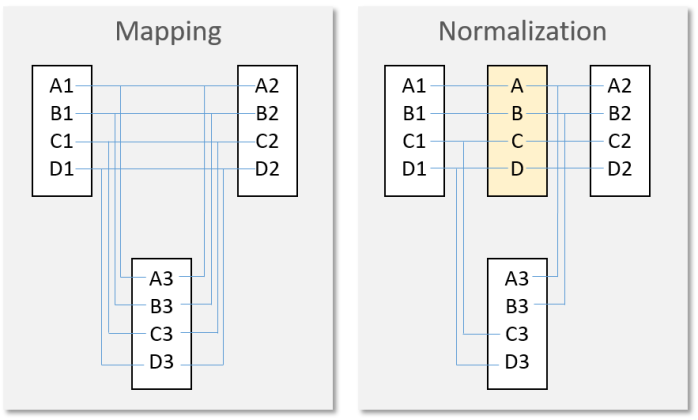
The following diagram illustrates this scenario.
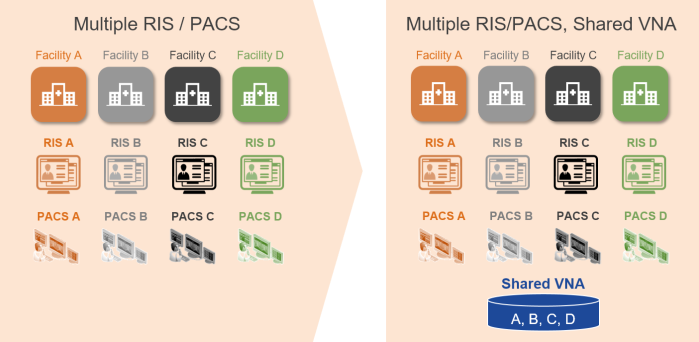
In this deployment, the shared VNA typically maps or normalizes procedure terminologies in the DICOM header of the studies that are served to the individual PACS systems as part of the relevant prior pre-/push-fetch workflows.
Single PACS, Single RIS
An increasingly common scenario is when health systems include a RIS consolidation project within their EMR consolidation strategy, while PACS consolidation happens in parallel. This approach results in a single master set of orderable procedures that is used by all participating facilities. The challenge arises from the fact that historic imaging records maintain, in the DICOM data, procedure information using historic terminology values that predate consolidation and can include known values (from the latest RIS) or some potentially unknown value (previous RIS systems for the institutions that replaced their RIS system at least once and did not replace the values with one used by the new RIS).
The following diagram illustrates this scenario.
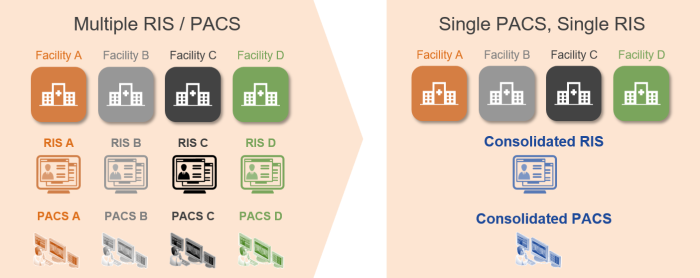
In these deployments, the consolidated PACS is responsible for dealing with new common and fragmented historic procedure terminologies.
In the next post, I will describe how PACS and VNA vendors deal with this challenge.