Radiology Information Interoperability for Productivity and Quality
In the early days of Radiology, data entry errors by Radiology Technologists (aka Techs) were common. Their attention was on the patient and the operation of the modality, not the clerical task of typing in data, after all. To address this, something called a DICOM Modality Worklist (aka DMWL) was developed and adopted.
Essentially, this took the textual patient and imaging procedure order information entered into the HIS or RIS (i.e. the order placer), and sent it to some system as an HL7 ORM message (an order). The structured patient/order information was then provided to modalities using the DICOM protocol (because this is the language they speak). DMWL could be provided by the RIS or PACS or some form of broker system that spoke both HL7 and DICOM.
This allowed trained clerical workers (or physicians), combined with software that validated the data entered (where it could), to pass the information to the modality workstation where it could be mapped into DICOM objects, without having to ask Techs to enter this info. The productivity and information quality gains were significant.
It is worth noting that the order provides other value than just eliminating duplicate data entry. It represents a work instruction, and it is used in scheduling and billing. Where image acquisition is not scheduled or billed for, orders are typically not created.
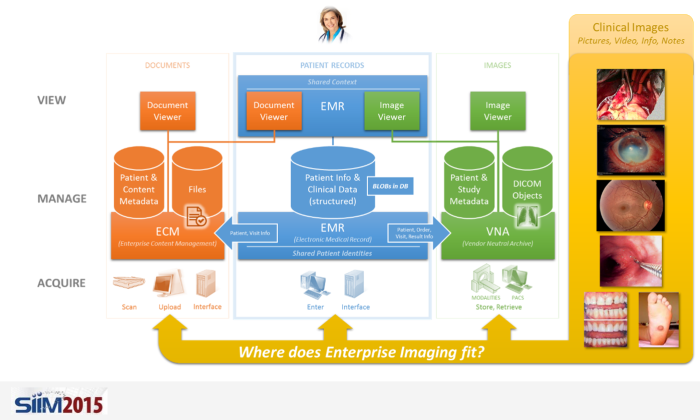
Enter Enterprise Imaging
As we enter the era of Enterprise Imaging, there are lots of lessons that we can learn from the solved problems in areas like Radiology.
For example, when capturing a photo in a Wound Care clinic, it has to be associated with the correct patient (obviously), but there is likely other pertinent info that should be captured, such as the anatomical region imaged and any observations by the physician.
In Enterprise Imaging, orders are often not placed. In many areas, the imaging is often not the primary task, but one that used to support clinical work.
If orders are not placed, how can we at least provide the benefit of passing textual patient data to the image capture device or application to reliably associate patient (and perhaps encounter or procedure) data?
Even if orders are placed, most of the devices and applications used in Enterprise Imaging cannot accept an HL7 message and do not speak DICOM. Some form of broker would likely be required yet again.
Enterprise Information Interoperability for Enterprise Image Capture
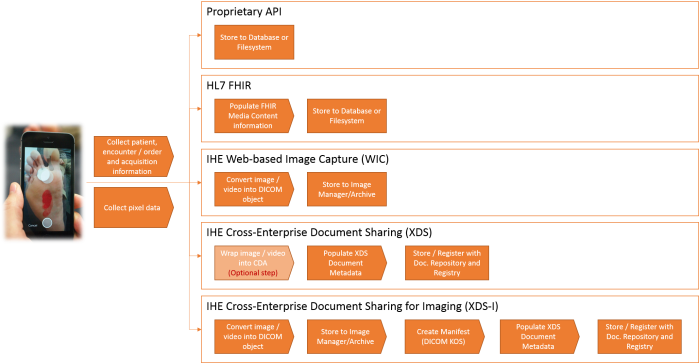
One hope that we have is the adoption of the new HL7 FHIR standard. Based on REST-based API design methods, it is much easier to integrate with different devices (especially mobile devices) than HL7 v2.x messaging and DICOM interfaces are. Other methods used are to generate a URL from the EMR, with all the info provided in parameters, that launches the image capture application/device in context. Another method is to use HL7 messaging to populate the VNA database with patient, encounter and order/procedure information (essentially a copy of what the EMR has), and use a tool or API (perhaps the DICOMweb™ Query API, QIDO-RS) to query this system to get the necessary information.
Don’t Forget the Metadata and Supporting Information
This still leaves the issue of how to reliably and consistently capture the information that goes with the image(s)—notes, anatomy info, findings, technical exam info, observations, etc. In DICOM, when this type of information is needed, a SOP Class is defined. The header of the SOP Class object specifies where all this metadata should go. This is one of the primary principles of interoperability: a defined format and data scheme, with a clear and shared meaning.
Assuming that not all Enterprise Images will be generated in, or converted into, DICOM format, the definition of the metadata schema may be left to be defined by the implementing vendor.
In addition to the clinical and technical data, sooner or later, someone is going to be looking for operational data for use in analytics and process improvement, so it will need to be captured (on some level of detail), as well.
Consistent Terms
And, even when we have a common schema, if the terms used within the scheme are not consistent, we end up spending an enormous amount of time doing mappings or integrating terminology services (and even then, never fully addressing all cases).
To Acquire or Not to Acquire
If we think about Enterprise Imaging that is not “ordered”, what triggers the acquisition of an Enterprise Image? Is it up to the clinic or individual care provider to make the judgement? Should a published set of best practices define this? Would the EMR have logic, based on the patient’s condition or care pathway, to prompt or force the user to acquire and store the image(s)?
Enterprise Imaging Acquisition Protocols Needed?
If we consider the different ways that images can be captured (still, video), the subject in frame (cropping, zooming), lighting, etc., and the ability to capture a single image or a set of images, do we also need some form of a book of protocols to guide the person acquiring the images? Should certain images contain a ruler (or object of known size) to allow the image to be calibrated for measurements?
The Cost of Doing Nothing
If we consider the impact of not having methods to avoid data entry errors, or not having a common schema, not having common terms, and not even having a common communication protocol or best practices for acquisition workflows, what hope does Enterprise Imaging have?
Even with options for all these things, imaging and information devices are still struggling to be interoperable with departmental and enterprise applications, as described in this Healthcare IT News article, “Nurses blame interoperability woes for medical errors”.
The Future is Now(ish)
This is why the mission and output of the joint HIMSS-SIIM Enterprise Imaging workgroup (charter in PDF here) is so important. The space needs to be better defined, with acquisition workflow practices, data formats, schemas, terms, and protocols outlined.
If we simply try to copy what is done in Radiology into Enterprise Imaging, it will create too much of a burden on the people asked to capture these images, and they won’t do it, frankly. Unlike the reimbursement in Radiology, they often have little incentive to spend the extra time to capture, index and upload images to the EMR when they are focused on the patient.
But, if we ignore the benefits that come with the controls and methods we have developed and matured over the years in Radiology, we risk having to re-learn all the same lessons again. And that would be very sad (and expensive, and wasteful, and unsafe…).
Add on top of all this the increasing need to share this data across different enterprises for continuity of care and the importance of interoperable data portability/liquidity is critical.
The fundamental healthcare informatics knowledge and business analysis skills developed by imaging informatics professionals, through on-the-job experience and membership in educational/research societies like SIIM, will be important in determining the right mix of proven concepts that apply, and new methods and innovations. Without a supply of talent to foster the change, nothing will change.
In Conclusion…
When dealing with such an undefined space, people often relish the idea of “doing it right this time”. I would urge anyone involved in this space to reflect on what has been accomplished in mature fields like Radiology, as there are a lot of “right things” that we may be taking for granted. With a little modernization, we can still get continued value out of what we have already achieved.