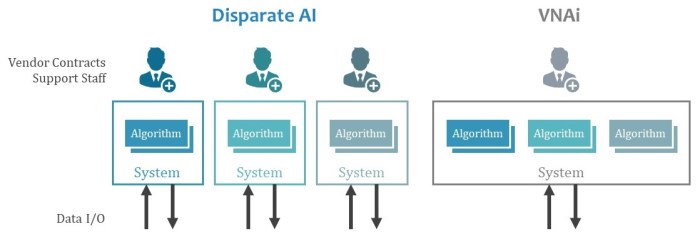
As health systems acquire or partner with previously independent facilities to form Consolidated Enterprises, and implement a Shared Electronic Medical Record (EMR) system, they often consolidate legacy diagnostic imaging IT systems to a shared solution. Facilities, data centers, identity management, networking equipment, interface engines, and other IT infrastructure and communications components are also often consolidated and managed centrally. Often, a program to capture and manage clinical imaging records follows.
Whether the health system deploys a Vendor Neutral Archive (VNA), an Enterprise PACS, or a combination of both, some investment is made to reduce the overall number of imaging IT systems installed and the number of interfaces to maintain. An enterprise-wide radiation dose monitoring solution may also be implemented.
While much has been written on strategies to achieve this type of shared, integrated, enterprise-wide imaging IT solution, there are several other opportunities for improvement beyond this vision.
In addition to imaging and information record management systems, enterprise-wide solutions for system monitoring, audit record management, and data analytics can also provide significant value.
Systems Monitoring
Organizations often have some form of enterprise-level host monitoring solution, which provides basic information on the operational status of the computers, operating systems and (sometimes) databases. However, even when the hosts are operating normally, there are many conditions that can cause a solution or workflow to be impeded.
In imaging, there are many transaction dependencies that, if they are not all working as expected, can cause workflow to be delayed or disabled. Often, troubleshooting these workflow issues can be a challenge, especially in a high-transaction enterprise.
Having a solution that monitors all the involved systems and the transactions between them can help detect, prevent, and correct workflow issues.
Audit Record Management
Many jurisdictions have laws and regulations that require a comprehensive audit trail to be made available on demand. Typically, this audit trail provides a time-stamped record of all accesses and changes to a patient’s record, including their medical images, indexed by the users and systems involved.
Generating this audit trail from the myriad of logs in each involved system, each with its own record format and schema, can be a costly manual effort.
The Audit Trail and Node Authentication integration profile (ATNA), part of Integrating the Healthcare Enterprise (IHE), provides a framework for publishing, storing, and indexing audit records from different systems. It defines triggering events, along with a record format, and communication protocol.
Enterprises are encouraged to look for systems that support the appropriate actors in the ATNA integration profiles during procurement of new IT systems and equipment. Implementing an Audit Record Repository with tools that make audit trail generation easy is also important.
Data Analytics
Capturing and analyzing operational data is key to identifying issues and trends. As each system generates logs in different formats and using different methods, it often takes significant effort to normalize data records to get reliable analytics reports.
Periodic (for example, daily, weekly, or monthly) reports, common in imaging departments for decades, are often not considered enough in today’s on-demand, real-time world. Interactive dashboards that allow stakeholders to examine the data through different “lenses”, by changing the query parameters, are increasingly being implemented.
Getting reliable analytics results using data from both information (for example, the EMR and RIS) and imaging (for example, modalities, PACS, VNA, and Viewers) systems often requires significant effort, tools to extract/transform/load (ETL) the data, and a deep understanding of the “meaning” of the data.
Enterprise Insight
Implementing solutions that continuously and efficiently manage the health of your systems, the records accessed, and operational metrics are important aspects in today’s Consolidated Enterprise. Evaluating any new system as to their ability to integrate with, and provide information to, these systems is recommended.