The SIIM 2018 Annual Meeting in Washington D.C. is just around the corner (May 31 to June 2). I look forward to seeing many friends, sharing ideas, and learning. I will be involved in number of sessions this year. Here is a preview.
Preparing for a Successful RFP and Contract with Vendors
Thursday, May 31 | 9:45 am – 10:45 am | Annapolis 1
In this roundtable session, participants will discuss how to best prepare for, develop, and issue an RFP, as well as how to analyze and grade the responses. We will also discuss how to best prepare for, and support, contract negotiations with a vendor.
Debate: Enterprise PACS vs. Vendor Neutral Archive (VNA): Choose Wisely
Friday, June 1 | 9:45 am – 10:45 am | Cherry Blossom Ballroom
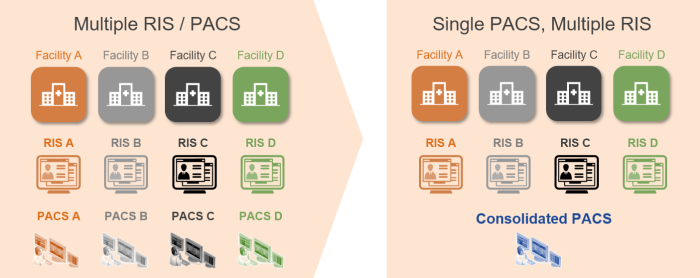
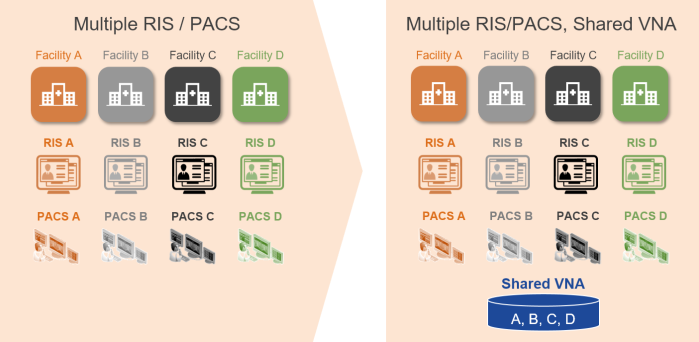
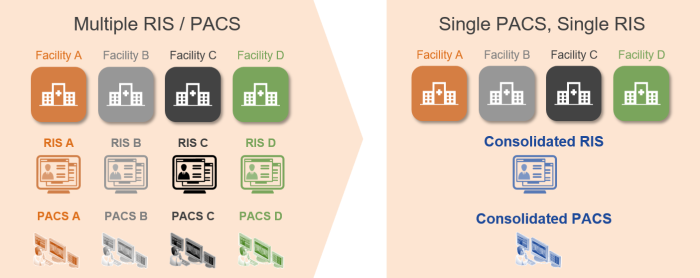
Depending on your organization’s goals and scale of enterprise, the options available to you for an image archive can vary. In this debate-style session, we will explore the merits of using a Vendor Neutral Archive (VNA) vs. an archive provided as part of an Enterprise PACS. I am moderating the session.
Imaging IT Financials – Learn from the Masters
Saturday, June 2 | 12:45 pm – 2:45 pm | Baltimore 3/4/5
Participants that sign up for this learning lab (limited seats available) will work hands-on with experts to learn how to perform clear and compelling financial analysis. Two lab exercises—one focused on assessing cloud-based vs. on-premises image archive storage, and another on the IT investment required for rolling out the enterprise imaging solution to a newly acquired facility—will be worked on in teams. Each team will share their work with the other near the end of the session. Lab assistants will be on-hand to assist. Participants must bring a laptop or tablet with Microsoft Excel installed.