Based on discussions with colleagues and our clients, Enterprise Imaging is becoming an integral part of U.S. Hospital IT Consolidated Clinical Record strategies.
HIMSS-SIIM Enterprise Imaging Workgroup‘s current working definition of Enterprise Imaging is as following:
- Diagnostic Imaging – Encompassing traditional diagnostic imaging disciplines such as Radiology and Cardiology
- Procedural Imaging – Including images that are acquired for diagnosis or clinical documentation purposes (such as visible light photos, point-of-care ultrasound)
- Evidence Imaging – Including images and/or videos that are acquired for clinical documentation purposes (for example, scope videos, computer aided detection)
- Image-based Clinical Reports – Documentation that includes or entirely consists of images (for example, Pulmonary Functional Test (PFT) report, multi-media pathology report)
Despite the attention from vendors, industry focus, and provider demand, this market space is still in its early stages of development. There are two main reasons: 1) the scope of the problem domain is still being defined; and 2) the vendor community is still working out the best practices and optimal technical approaches.
Moreover, the number of the departments that generate Enterprise Imaging content and that have their own departmental workflows is quite large.
This results in significant confusion on the provider side who are left to navigate a myriad of perspectives expressed by the imaging informatics industry. There are on-going initiatives that are currently working on demystifying the field of Enterprise Imaging. For example, the recent SIIM Webinar delivered by Dr. Towbin from Cincinnati Children’s, provides a very thorough analysis of the problem domain.
In conversations with vendors and providers, we have compiled several observations that might benefit the imaging informatics community.
The Right Approach
In the SIIM 2015 Opening General Session presentation, Don Dennison presented the following slide titled “Enterprise Image Management: Making the Right Choice”
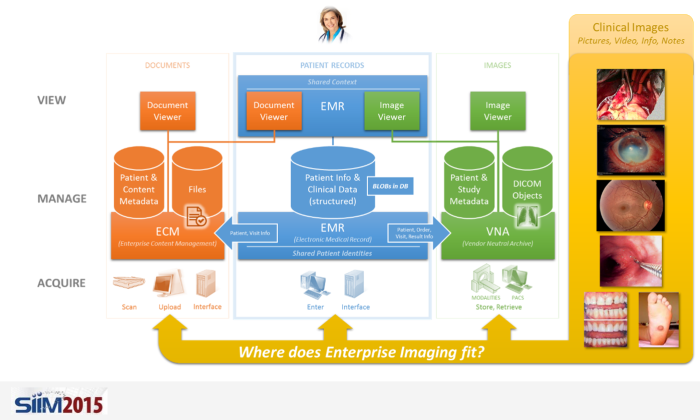
With the various systems in place to manage patient record data, there is often debate as to which enterprise system is best suited to offer Enterprise Imaging services.
At the moment, there is no obvious answer to the question presented by the slide. Besides the technical capabilities of the systems, the provider’s internal IT capabilities, capacity and policies can significantly influence the decision. At some organizations, where the Imaging Informatics Team plays a prominent IT role, the choice could be the VNA, while at others, where the Enterprise IT team takes the lead, the EMR or ECM is often chosen.
The Right Functionality
During RSNA 2015, we conducted a study to identify the state-of-the-art of Enterprise Imaging technology, including methods of acquisition, management, and distribution of non-DICOM images. The following table summarizes our findings.
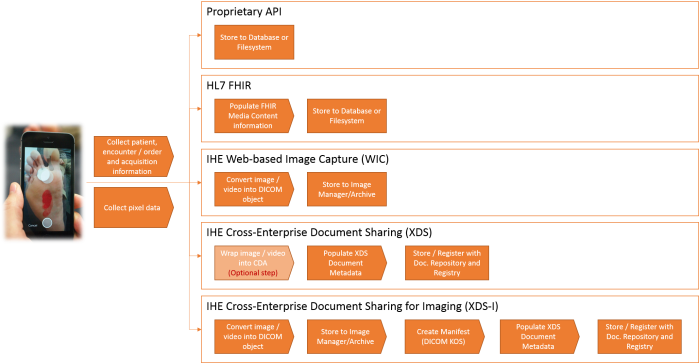
| Image / Video Acquisition |
| Ability to capture from mobile devices |
The majority of current vendors opted for native applications to provide better user experience and tighter security controls. Still, image capture is the prevailing capability, with video acquisition capabilities lagging behind. Some vendors offer integration with leading EMRs’ mobile applications. |
| Ability to capture from visible light cameras |
The ability to manually (i.e. file browse, drag & drop, etc.) upload both videos and images is a commodity. Automatic ingestion, on other hand, varies significantly from vendor to vendor. Most vendors offer proprietary integration frameworks, but their comprehensiveness and real-life integration experience is very different from one to another. |
| Ability to capture from different scopes |
Most of the vendors leverage third party hardware devices to integrate with digital or analog video sources real-time. |
| Acquisition Workflow |
| Order-based Workflow |
DICOM Modality Worklist (DMWL) SCU support, as well as the ability to generate or receive order information, are available in most vendor’s applications.
Context-based launch of the capture application is also a well understood and supported functionality.
Many of the vendors mimic an order-based workflow (i.e. create the Accession Number) for the acquisitions that are not scheduled. The main challenge with this approach is to determine the correct method to feed the created information back to the EMR (e.g. often called an “unsolicited result”, which may not be supported at the site). |
| Encounter-based Workflow |
Some vendors, originating from the Diagnostic Imaging space, struggle with native Encounter-based workflow support.
On many occasions, departmental visit/encounter information, supplied in HL7 messages from the EMR, is sufficient to build specific acquisition worklists for different service lines. |
| Scenarios where information services are not available |
Most of the vendors offer the ability to manually create patient and procedure information. The difference lies in whether all or just a sub-set of capturing methods (e.g. mobile vs. desktop) support that functionality. |
| Patient identity management |
Standards-based methods to discover or receive patient information is widely supported, while the support for proprietary methods to connect to patient information sources varies from vendor to vendor. |
| Ability to Edit Images/Videos |
| Editing Tools |
Most of the vendors rely on an installed Windows OS client application to edit (e.g. crop) acquired images or videos as part of the manual upload process (e.g. drag & drop). Selected vendors also allow static image editing only (i.e. no video) during the mobile capture. |
| Images |
An ability to associate different types of metadata (including notes) is supported by the majority of the vendors. Also, basic manipulation of the acquired images such as image deletion, markups and annotation, which are stored as overlay objects associated with the acquired images is common.
Only selected vendors are capable of calibrating images on-the-fly by using recognizable objects of known size embedded in the image. |
| Videos |
A flexible and comprehensive ability to associate different types of metadata (including notes and keywords) is supported by the majority of the vendors.
Most of the vendors have very limited (if at all) video editing and capturing capabilities and rely on third party providers. |
| Viewer |
| Current state |
The solutions typically consist of the following viewers:
- Mobile capture
- Desktop image/video upload
- Desktop image/video editor
- Zero-footprint (ZFP) EMR viewer with very limited, if at all, editing capabilities
|
| Privacy and Security |
| Current state |
Most of the vendors offer a range of methods to ensure PHI protection such as:
- Information deletion/encryption from the device
- Strong Authentication and Authorization methods
- Auditing
|
| Reporting |
| Current state |
The most prevalent approach is to rely on an external system, such as the EMR or specialty-specific reporting application, to create and manage reports. |
| Record Management |
| Current state |
Most of the vendors opt for managing image and videos in their native format, while converting the content on-the-fly for standards-based communication with external systems. |
Conclusion
It seems that Enterprise Imaging is going to rapidly evolve and we are eager to see how our clients, and providers in general, will benefit from these changes.
Working on an Enterprise Imaging project? Leave us a comment with your thoughts, or contact us.