Brad Genereaux, co-chair of DICOM Working Group 27, posts on how to drive developer adoption.
Definitely worth a read (be sure to follow him if you work in healthcare IT).
Brad Genereaux, co-chair of DICOM Working Group 27, posts on how to drive developer adoption.
Definitely worth a read (be sure to follow him if you work in healthcare IT).
I started writing this blog post about this…
Opinions on policy and politics aside, this article on the struggles of healthcare.gov tells a classic tale of large software development project failures, and how not to react when trying to solve the issues.
But as I continued to write my thoughts, this became more about my views on software development and crisis management. So, enjoy (or ignore, or comment).
Hopefully, it is worthy of my 100th blog post (which this is).
On software development…
On crisis management (in IT)…
And, finally, if you are making an application for use in healthcare, take it seriously. Lives are at stake. It can still be fun and rewarding, but the problems within healthcare are large and demand our best efforts all the time. Now, go be great.
I posted some thoughts recently about an article on impact of privacy on patient record sharing.
Now, here is an article that discusses the merits of giving the patient control over how they are identified and how their records should be shared.
Fundamental to this are the two approaches:
Some thoughts…
As this article explains, the rules of accountability need to apply to all parts of the delivery chain, from the healthcare provider to the infrastructure vendor.
It is my experience that the readiness of the vendor to provide the necessary security controls (technical, policy, etc.) is usually not the issue. It is often the healthcare provider staff that lacks the knowledge of appropriate and effective controls that prevents proper security from being in place.
For example, even when proper single sign-on (SSO) methods are available in systems, rather than taking the time to implement this between systems (which often requires some learning), staff will often default back to wanting to simply pass a user ID and password (often a generic one) from one system to the next, because that was all they could do 10 years ago to avoid having the user log into multiple systems.
Not really related to healthcare IT, but an interesting read. Shared by a friend.
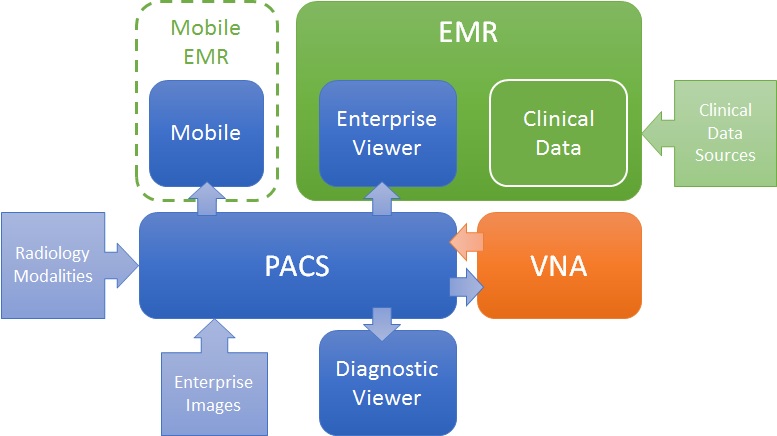
Like many problems, there are more than one valid solution. For the challenge of getting images to both diagnostic consumers (e.g. Radiologists) and clinical consumers (e.g. ordering physicians, EMR users), there are many ways to define a solution architecture, but two are most obvious: PACS-centric and VNA-centric.
PACS-centric
In this model, the PACS is the primary system, interfacing with modalities, providing a client to diagnostic users, as well as access to clinical users though an enterprise client embedded in the EMR. Mobile access may be direct or via a mobile EMR user interface, but it is getting images from the PACS. Enterprise images are captured and stored in the PACS (though storing to VNA and routing to PACS is also possible). The VNA’s role is primarily as an archive to (one or more) PACS.
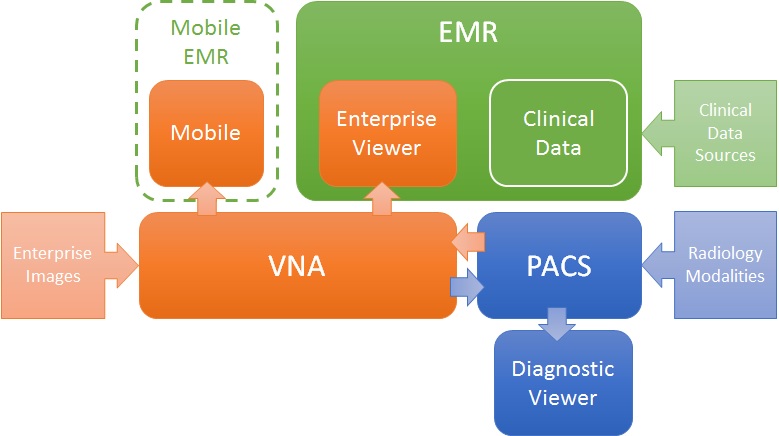
VNA-centric
In this approach, the VNA is the primary image management system. The PACS likely still interfaces with modalities (though not always), but captured enterprise images are stored to the VNA, and sent to the PACS when needed/supported. Clinical viewing in the EMR is done by an Enterprise Viewer, which may or may not be provided by the VNA vendor. Mobile access is also through the Enterprise viewer, getting images from the VNA.
Pros and Cons
As stated, both are valid approaches, but each has some inherent strengths and challenges.
The PACS-centric solution has a high likelihood of having all parts of the medical imaging record being available in both diagnostic and enterprise viewers. Proprietary data (e.g. markups and key images) not provided through standard data objects (e.g. DICOM GSPS and KOS) are more likely to be visible in all clients. There may also be some common application configuration settings across clients, which would reduce administration complexity and cost. Getting the image management and image viewing (diagnostic and enterprise client) all working together is the burden of the vendor (i.e. it is an engineered solution designed to function as a single system).
The VNA-centric solution is better suited to support a multi-PACS environment, providing a common management and viewing platform for enterprise users—only the single Enterprise Viewer is embedded in the EMR (vs. the multiple ones provided by each PACS). Environments with multiple PACS and Mini-PACS benefit as the VNA is the common sharing (and data quality validation) point among them—this allows for a more “pluggable” solution where systems that address niche needs can be used until the primary PACS is able to replace them. In this model, the integration among the components is more complex and places a higher burden on the institution to get it all working (i.e. the informatics and IT staff need to be willing and able to put this together), even with purchased professional services from all the vendors involved.
Assuming both the PACS and the Enterprise Viewer support LDAP (Lightweight Directory Access Protocol) and/or SSO (Single Sign-On), user authentication may be equal in both approaches.
Both a well-designed PACS and VNA (and Enterprise Viewer) can provide effective multiple patient ID management methods (e.g. MPI or IHE Patient Identifier Cross-Referencing), to allow integration/exchange of patient imaging records across patient ID domains, though the VNA and Enterprise Viewer are traditionally more likely than PACS to support flexible models.
In both models, storage for the long term archive is expanded at the VNA.
For years, I have heard providers lament at the slowing (dormant?) pace of innovation in PACS and RIS from established vendors.
Why might this be happening?
It could be that the current architectures have reached their limits. It could be that, with the saturation of PACS in mature markets, vendors are reducing R&D investment in this area. It could be that they can’t sustain the talent needed to innovate, losing creative and skilled people to more interesting/promising areas of IT. It could be innovation-suppressing regulatory burdens. Or the shift of spending to support staff in order to sustain the now sprawling installed base.
Regardless of the root cause(s), I see the emergence of interest in start-ups (such as those in the SIIM Innovator Alley) and open source projects (as seen by the steady traffic at the SIIM Open Source Plug Fest) that attempt to solve problems that the larger vendors appear not to be interested in solving. It seems providers are starting to accept that they are not going to get everything they need from their incumbent PACS vendor in today’s EMR-enabled, Cloud-hosted, analytics-driven, enterprise-accessible market.
Of course, the challenge of the start-up is breaking into the provider’s enterprise where the incumbent vendor may put up some resistance (overtly or passively). And open source is only as good as the staff (or paid service provider) you have installing, integrating and supporting it.
The informatics skills and knowledge provided by SIIM are more important than ever. If SIIM is to continue to lead in providing its members the knowledge and skills they need to survive and succeed, it will likely have to adapt how it organizes the materials to align with new and evolving learning goals. It also needs to adapt the medium by which its members learn, providing focused, on-line options where travel policies and budgets mean attending the annual meeting is not feasible.
I believe in the SIIM strategic plan and am wholly committed to helping the society that has helped me so much over the years thrive.
Another great SIIM annual meeting is behind us and it was great, as always. I am going to post some thoughts and reflections this week.
Today, I have been thinking about analytics and, in particular, the use of a workflow engine and a standardized set of terms and definitions (such as what is being defined in SWIM) to ensure analysis of workflow events (type, timing, relationships, patterns, etc.) consistently across systems.
There were several great talks by Dr. Brad Erickson and Chris Meenan and others on the topic and these were followed by a large turnout of engaged attendees for a SWIM demo (see pic below).
My thoughts…
More thoughts from SIIM later. Stay tuned.
I find the topic of this article interesting.
Here’s why…
Check out this article. Some fairly common observations for an IT veteran, but good advice for EHR buyers.
Some mitigation tips for each point (read the article for the 4 hurdles)…
In regards to the comments on the trade off of lost productivity vs. potential new revenue, check out this post from a month ago.
