I play Fantasy Football. Usually very badly. For those that don’t know about this hobby/addiction, this will explain it.
Why am I talking about Fantasy Football on a blog about healthcare IT? Because an intriguing feature showed up this year (I have been in the same league since 1998) on the site that manages our league.
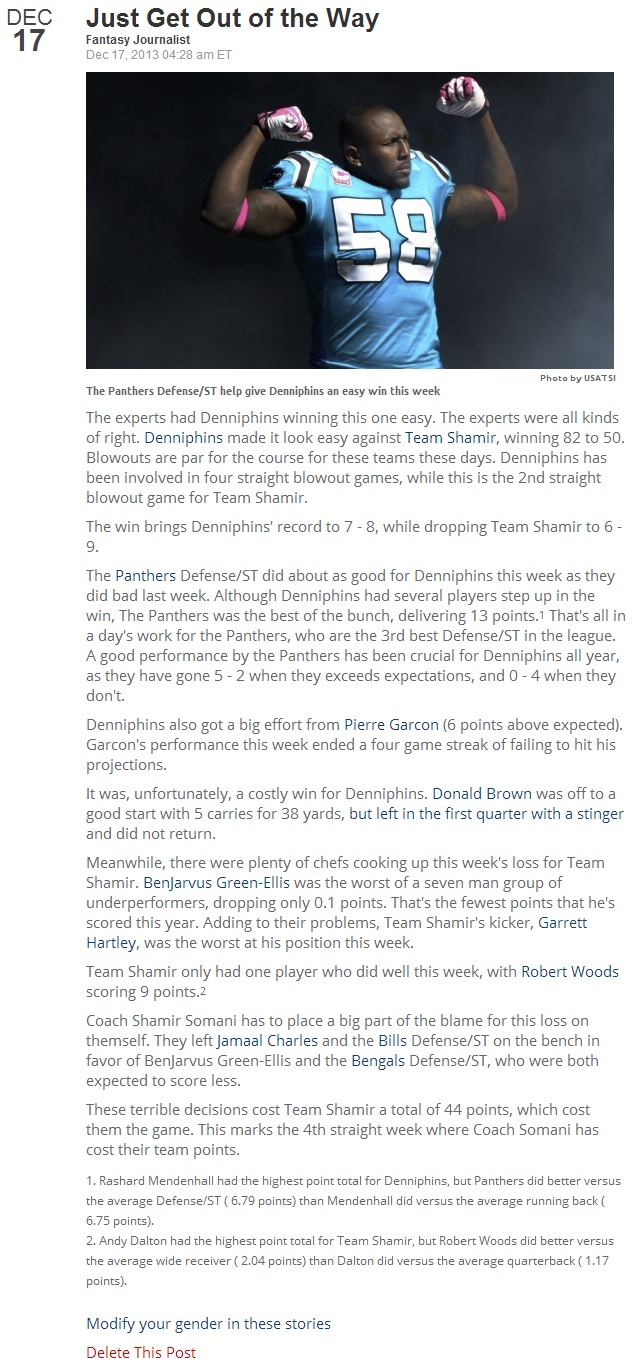
After each week, an article describing the battle between my team and my scheduled opponent’s team appears. It is well-written, insightful and sometimes entertaining. The thing is: it is not written by a human.
The quality of the writing is what makes this interesting. You wouldn’t know that a trained journalist had not written the article unless you knew that a computer did it. Take a look at the image below and tell me that sounds like a computer wrote the article pictured within it.
(BTW, for those Fantasy Football fans that read the article, I missed the playoffs, so the victory described is hollow …I really am terrible at Fantasy Football).
Considering the uniqueness of the scenario—the odds of exactly my 9 starting players playing my opponent’s starting 9 players are extremely rare considering the hundreds of players to choose from, even considering there are tens of millions of leagues operating on the site (yes, Fantasy Football is that big)—the text of the article is highly personalized.
Back to healthcare IT, and how this relates.
Consider the wealth of structured clinical data and diagnostic findings that could be combined with genomic data to produce an information model of a patient. Now consider that an application could take that information and automatically turn it into a narrative report that is optimized for different consumers—for example, one for the GP, one for the specialist, one for the patient, one for the home-based caregiver, etc.
Hyperlinks could make extended clinical or reference data available with the press of a finger.
Obviously, a qualified healthcare professional needs to review and sign/finalize the results before they should become part of a patient’s medical record, but imagine how the report could become more useful to the reader, if tailored to their needs, and how much typing and editing could be saved.
Once all this patient data is unlocked using secure REST-based APIs, like those defined in HL7 FHIR and DICOMweb, some very powerful applications can emerge and revolutionize how results are created.
The interpretation of the images is the high value add that Radiologist provide, not typing or dictating—why not free them up to spend more time with their eyes on the pixels and let the computer do the typing?
Inspiration for innovative solutions to problems comes from all types of places. You just have to look for it. 🙂
Figure 1 – Rare example of A Fantasy Football victory